
Have you been wondering how much money US doctors made in 2020? It was, after all, a year marked by one of the worst health crises in modern history – the COVID-19 pandemic. The impact on our healthcare system has been profound, including impacts on physician compensation.
Not only were hospitals inundated with extremely ill patients in certain parts of the country but their most lucrative source of income, elective surgeries, evaporated overnight.[mfn]1[/mfn] This affected everyone who works in hospitals, including surgeons, radiologists, and other hospital-based-physicians.
Furthermore, visits to primary care doctors dropped precipitously as we were confined to our homes.[mfn]2[/mfn] And, the fear of catching COVID at our doctor’s office scared the bejeezus out of many. Even oncologists and other specialists experienced patients staying away even when they urgently needed the care.[mfn]3[/mfn]
Related content: Poor Payer Reimbursement and Practice Viability during COVID-19
Doctors and other healthcare workers found themselves in an unexpected situation with drastic declines in income and even work furloughs.[mfn]4[/mfn]
Interestingly, but not surprisingly, the healthcare sector responded to these threats with innovations that helped turn the financial calamity around. Telemedicine was rapidly instituted.[mfn]5[/mfn] And, strict procedures were implemented to make surgeries and visits to the doctor’s office safer.[mfn]6[/mfn] Patients were reassured to see their providers wearing masks and face shields.
So, what has been the net effect of all of this on doctor’s incomes year-to-date? Let’s take a look.
The 2020 Doximity Physician Compensation Report
Doximity is the largest professional network in the US having more than 70% of all U.S. doctors as members. They have been collecting data from survey responses from 135,000 licensed US physicians over the past six years. This is the fourth year that they have published a Physician Compensation Report.
According to one of the lead authors of the story, Peter Alperin, M.D., a practicing internist and the Vice President of Product at Doximity, this survey differs from other physician compensation reports in two important ways:
- The number of licensed physicians participating in the survey is larger
- All of the physicians who participated are verified to actually be licensed physicians
Here are the key findings:
-
Physician compensation growth was relatively flat overall
Compensation growth was only 1.5% according to this year’s report. This is quite modest compared to increases of up to 4% in previous years. Further, because the 2019 inflation rate was 2.3% (as measured by the Consumer Price Index)[mfn]7[/mfn], it suggests that physicians overall had a decline in real income.
-
There’s a big difference between the highest and lowest compensation by metro area
There is more than a $100,000 difference between the metro area with the highest compensation (Milwaukee – $430,274) and the area with the lowest (San Antonio – $329,475). But it’s hard to know what this really means because there are many factors that contribute to the calculation of “average” compensation, including:
-
-
-
- Specialty mix
- Gender mix (more on that later)
- Physician age mix
- How much rich benefits compensate for lower salaries
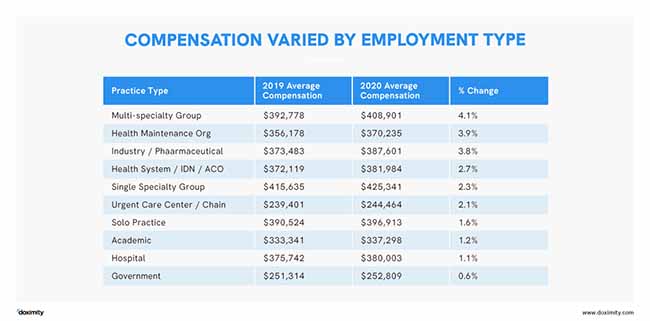
The report provides some detail on another important factor impacting compensation: employment type. -
-
-
Physician compensation doesn’t track with the cost of living
It is interesting to note that metro areas with the highest cost of living [mfn]8[/mfn] do not appear on the list of places with the highest compensation.
That speaks to the fact that there are other considerations besides compensation and the cost of living that physicians may take into account before they pack their bags and move to Milwaukee. These include:
-
-
-
- The desirability of the area for their and their families preference (e.g., must live near an ocean to surf, can’t stand cold winters or hot summers)
- Availability of good schools and safe neighborhoods
- The presence of an academic medical center in the community is important to some physicians
- Nearness to extended families (especially important when the physician family includes children)
- Diversity of the population
- Proximity to a major international airport to make travel easy
- The richness of the culture and arts scene
- Availability of good restaurants, bars, sporting events, recreational, and cultural activities (we are not going to be sequestered forever)
- Politics (liberal vs conservative)
- Religious factors (availability of communities with similar beliefs
-
-
I could go on and on, but you get the picture. Compensation is important, but it isn’ everything.
-
Metros with the highest growth rate in compensation
Providence, Rhode Island tops the list with an 8.9% growth rate followed by Portland, Oregon with 8.6%. Again this is hard to interpret because so many different factors contribute to how rapidly compensation increases (shortages of physicians, insurance status of patients (and more). So I will just leave it at that.
Compensation by specialty
The single most important decision a medical student makes is what specialty training to pursue. You have to start applying for residencies in your 4th year. However, you may have had to arrange rotation opportunities to position yourself to get a coveted residency long before that.
There is no question that potential future earnings may play a role in some of those decisions, luring soon to be newly minted doctors into highly compensated specialties. It may also discourage some medical students from choosing the lower-paying specialties, particularly if they are staring a $100,000 or more in student loan debt.
So what did the report show about who makes how much?
The highest compensated medical specialty is neurosurgery
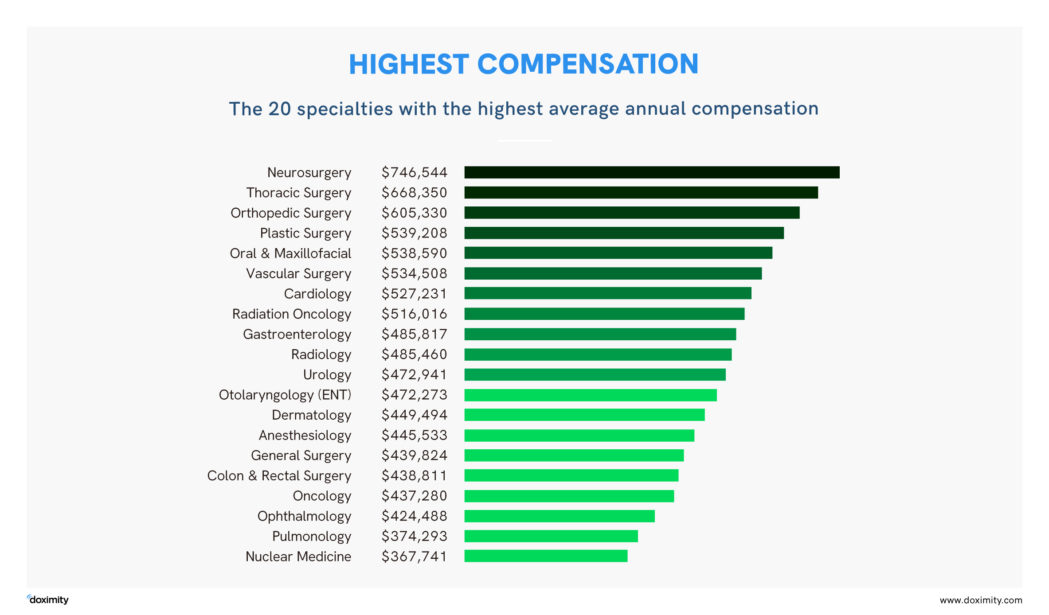
Primary care specialties are among the lowest compensated medical specialties

The gender wage gap
Sadly, the report documented a 28% wage gap between male and female physicians. This is up from 25.2% last year. We have been arguing about why there is a wage gap ever since I got into medical school as a result of the women’s movement that swept the country in the 70s. This is what I have heard about this topic my whole career:
-
-
- Women physicians don’t work as long and hard as men
- Women choose* the poor paying specialties (pediatrics and primary care) whereas men choose more lucrative surgical specialties, such as neurosurgery and orthopedic surgery. (*it is possible that gender discrimination may also have played a role in women’s choices. Some may have been actively discouraged from applying and others were simply not accepted in surgical subspecialty residencies.)
- Women choose salaried employment over the more “entrepreneurial” fee-for-service types of arrangements.
-
But this year’s increase in the wage gap may also reflect gender differences in the impact of the pandemic on the ability to continue working at the same intensity as prior to the shutdowns.
Schools closed down so daytime “childcare” evaporated. Kids were now home all day and many required help with online learning and even full-time homeschooling when online options were not adequate.
-
Women are usually called upon to make the sacrifice
Doximity’s Dr. Alperin, says that “women are usually the ones to called upon to make the sacrifice” if one parent must stay home to care for the children. In addition, because male physicians make more money than women physicians, they may feel that it makes sense for the family unit if the higher wage earner is the one to return to work
No matter that “we have come a long way, baby”, the bulk of these duties still fall to the moms of the house – even if she has a medical degree.
In fact, the widening of the wage gap between men and women has been reported in other industry sectors as well.[mfn]9[/mfn]
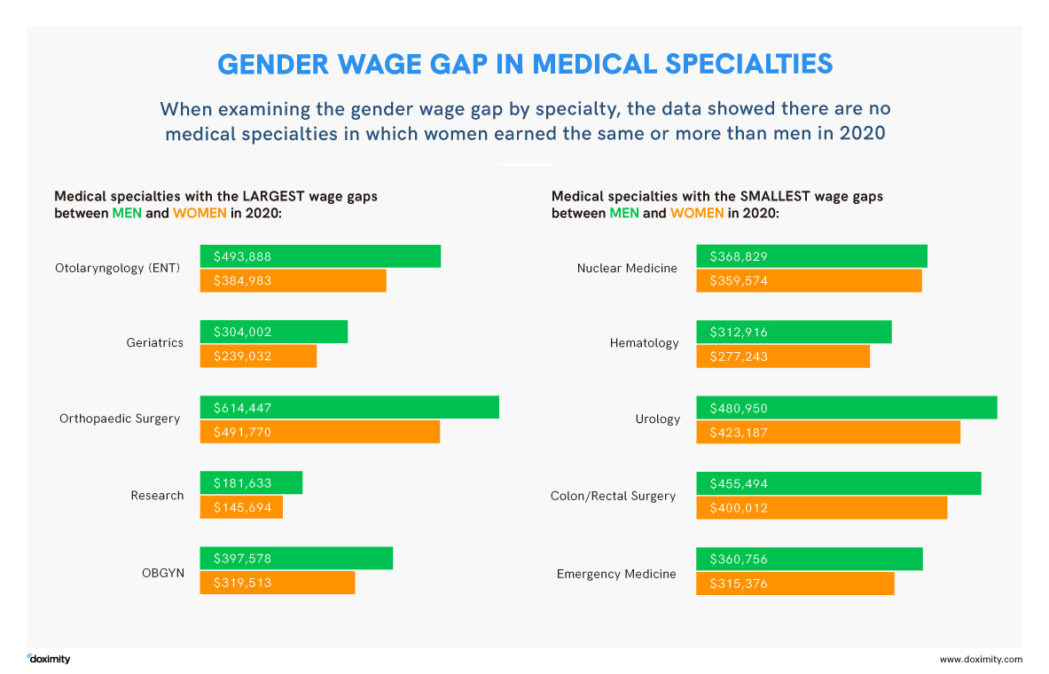
The gender wage gap by specialty
The report shows that there are no medical specialties in which women physicians earned the same or more than men. So even if women enter the higher-paying specialties, they still make less than their male colleagues.
The bottom line when it comes to physician compensation in 2020
Like many other people in the US, physicians took a financial hit because of the coronavirus pandemic. However, their compensation is still quite generous, placing many of them in the Top 10%. The most troubling finding in the report is the increase in the persistent gender wage gap in physician compensation. It will be interesting to see if this returns to “normal” once the pandemic is under control and life goes back to more or less normal.
References
1. ITIJ, US hospitals losing around $50 billion a month due to Covid-19. May 4, 2020. https://www.itij.com/latest/news/us-hospitals-losing-around-50-billion-month-due-covid-19
2. Rubin R. COVID-19’s Crushing Effects on Medical Practices, Some of Which Might Not Survive.
3. Papautsky E, Hamlish T. Patient-reported treatment delays in breast cancer care during the COVID-19 pandemic. Breast Cancer Res Treat 2020 Nov;184(1):249-254. doi: 10.1007/s10549-020-05828-7. Epub 2020 Aug 9.
5. Salber P. Doximity’s New Telehealth Application Makes It Easy to Connect, The Doctor Weighs In, June 3, 2020. https://thedoctorweighsin.com/doximity-telehealth/
6. Salber P. Clinical Care of Cancer Patients in the Age of COVID, The Doctor Weighs In, Aug 8, 2020. https://thedoctorweighsin.com/clinical-care-cancer-patients-covid/
7. U.S. Bureau of Labor Statistics, Consumer Price Index: 2019 in review. January 16, 2020. https://www.bls.gov/opub/ted/2020/consumer-price-index-2019-in-review.htm
8. Eastman S, Vazquez-Soto A. What is the Real Value of $100 in Metropolitan Areas, Tax Foundation 2020: https://taxfoundation.org/real-value-100-metro-2019/
9. New York Times, Pandemic Will ‘Take Our Women 10 Years Back’ in the Workplace. September 26, 2020. https://www.nytimes.com/2020/09/26/world/covid-women-childcare-equality.html
Methodology: Doximity used self-reported compensation survey data from 2019. and 2020 from ~44,000 full-time, licensed U.S. physicians who practice at least 40 hours/week. Responses were mapped across metropolitan statistical areas (MSAs). For more details, please refer to Doximity’s 2020 Physician Compensation Report.
Original article published in 2015. Updated 2/2/17. Updated 11/8/20.
Patricia Salber, MD, MBA
Website:
https://thedoctorweighsin.com
Patricia Salber, MD, MBA is the Founder. CEO, and Editor-in-Chief of The Doctor Weighs In (TDWI). Founded in 2005 as a single-author blog, it has evolved into a multi-authored, multi-media health information site with a global audience. She has worked hard to ensure that TDWI is a trusted resource for health information on a wide variety of health topics. Moreover, Dr. Salber is widely acknowledged as an important contributor to the health information space, including having been honored by LinkedIn as one of ten Top Voices in Healthcare in both 2017 and 2018.
Dr. Salber has a long list of peer-reviewed publications as well as publications in trade and popular press. She has published two books, the latest being “Connected Health: Improving Care, Safety, and Efficiency with Wearables and IoT solutions. She has hosted podcasts and video interviews with many well-known healthcare experts and innovators. Spreading the word about health and healthcare innovation is her passion.
She attended the University of California Berkeley for her undergraduate and graduate studies and UC San Francisco for medical school, internal medicine residency, and endocrine fellowship. She also completed a Pew Fellowship in Health Policy at the affiliated Institute for Health Policy Studies. She earned an MBA with a health focus at the University of California Irvine.
She joined Kaiser Permanente (KP)where she practiced emergency medicine as a board-certified internist and emergency physician before moving into administration. She served as the first Physician Director for National Accounts at the Permanente Federation. And, also served as the lead on a dedicated Kaiser Permanente-General Motors team to help GM with its managed care strategy. GM was the largest private purchaser of healthcare in the world at that time. After leaving KP, she worked as a physician executive in a number of health plans, including serving as EVP and Chief Medical Officer at Universal American.
She consults and/or advises a wide variety of organizations including digital start-ups such as CliniOps, My Safety Nest, and Doctor Base (acquired). She currently consults with Duty First Consulting as well as Faegre, Drinker, Biddle, and Reath, LLP.
Pat serves on the Board of Trustees of MedShare, a global humanitarian organization. She chairs the organization’s Development Committee and she also chairs MedShare's Western Regional Council.
Dr. Salber is married and lives with her husband and dog in beautiful Marin County in California. She has three grown children and two granddaughters with whom she loves to travel.





Comments:
Leave a Reply
Comment will held for moderation










I am very curious how other doctors see using their degree after Covid. For example, the author started a blog and ended up becoming nationally known and working in consulting along with getting an MBA. As an oculoplastic surgeon who spent almost three months unable to work and make any income my practice ended up accumulating quite a bit of debt and i think that is Not factored into this article in terms of revenue growth. However I started to think about how I could use my degree and what my other interests were. My mother was a writer for the Washington Post and an editor. Both sisters work in technical editing and have had fascinating careers. So because I do like to write and could see where I could do medical editing I started doing a technical editing certificate course of study at U. of Chicago. I got so interested in that, I started to think what if I wrote articles as well? Then I thought would I write about my own field? I thought no I wouldn’t. Because it would be all technical and frankly to me, rather boring. Then because I do like to learn, I read up on other fields of study and I became very interested in Epigenetics especially as it relates to disease and aging. I read up on Genetics, which I had always liked and then decided to do a Masters in Genetics at John Hopkins part-time online. So while I still am operating and changing parts of my practice- I also have a secondary plan that would allow me to retire and yet work from anywhere and possibly be a subject expert through the masters and my m.d. or lead to consulting or speaking. I wonder if other doctors have thought about how they could work remotely and retire into new fields with likely less pay, but far less overhead, stress and with new challenges. I ruled out an MBA because I’m not interested in Finance and frankly at this point in time in american history I am appalled at the response of average americans to education in Public Health and preventive care and just the overall respect for the medical field. I don’t know how this will change if the perception of doctors is tied to wages ( as it is in this article) and insurance companies, big pharma and even our own government dictates that perception to their own benefits in decreasing reimbursements- where is the incentive for that to change? How can we possibly have free healthcare in this country when it costs So much money for any young person to become a doctor? I see that having to change first. Plus we have a coming shortage of doctors as we do not have enough training programs. I want to contribute to society through being a doctor, I went to very good schools, and my twenties and most of my thirties went to training. Still I racked up enormous student loan debt and that most definitely factored in my choice to become a surgeon and ophthalmologist. My advice to young people is that if you do choose a surgical subspeciality because of perceived pay you shortchange yourself with later career choices. I would like to see more M.D, MPH’s and M.Ds, MBAs and underwriting of medical school costs by either the government, fair loans, or even medical corporation investing in future workforces. I would love to hear from the author about this, and any other doctor who has the same concerns. This is a real shift in medicine currently.
You are raising a few different issues. One is the perverse incentives (debt with the eventual promise of a lucrative career) that leads some medical students to choose high paying residencies. I do think that we need to tackle student debt head-on – getting rid of high-interest loan programs, perhaps replacing them with government-subsidized low-interest programs, like the National Defense Student Loan programs that made it possible for me to go to a four-year college.
The other issue you raise is how to stay happy and in love with medicine (https://thedoctorweighsin.com/career-in-medicine/) as circumstances change. You correctly pointed out that I have done many different things in my career, finding fulfillment in each of them. I moved around because that is what made me happy, kept me challenged learning new skills, and satisfied my endless curiosity. A close friend of mine did the opposite. She fell in love with GYN surgery early in her career. After her formal retirement, she found a part-time position at an academic institution where she can continue to operate and teach residents.
I think the important thing is to not feel stuck in something you no longer want to do no matter how great of an investment you made. Those are “sunk” costs. Be brave, explore, try new things out if you can. There are many ways to contribute to medicine and health care. It sounds to me like medical writing might be one of them. We should talk. Shoot me an email at [email protected].
In the spring most physician practices closed to all but emergency patients for several months, followed by a gradual reopening with restricted patient numbers due to appropriate distancing and disinfection measures. For most, gross medical practice income must have taken a severe hit. Rent, employee benefits, staff salaries, durable equipment costs all continued unabated. How is it possible that docs had a small increase in take home pay rather than devastating cuts?
I have just retired from a solo practice. The fee for service model that rewards procedures and of course the more you do the more you make is NOT a great way to allocate health care dollars. To provide a generous compensation to intelligent, service oriented, talented young people who are sacrificing years of their youth to work in medicine seems appropriate. Still if we are not to end up squeezed down by penny pinching every procedure we will need another model. This would upend the entire way of doing what we do. A Medicare for All system would not do this. It would overcome the disparity of socio-economic disparity and quality of health care and would significantly reduce the cost of our bloated system by eliminating the “middle man”. It would relieve our private sector the providing health care as most of their counterparts outside of the US don’t have that line item. The FEAR of government run health care is palpable in at least half of the american population who assume that “bureaucratic Death panels” will be deciding their fates. Of course corporate boards are benevolent and profit margins of denying coverage has never entered into the actualial decisions of these bureaucrats. We are going to need to address the health care disparity issue and the cost of health care including these compensation issues or we are going to see the “work harder for less and less” model screwing down the profession.
Hi Richard, thank you for your comment. I couldn’t agree with you more about the perverse incentives related to fee-for-service medicine. It is way past time to replace it with salary/bonuses/benefits. It is also high time that we join the rest of the developed world and provide health care coverage for everyone. That being said, I congratulate you on your retirement – enjoy! Pat
I have found, in over 27 years in Emergency Medicine, that many women back off when they have young children. 1. Many go to Urgent Care for better hours but less pay. 2. Many women with young children do not want to work nights, which, in many places, pays a premium. 3. Despite being “full time” do work fewer hours and may not get the same productivity bonuses. 4. Women are more likely to take a full 12 weeks for maternity leave, which does pay less than your salary. Many more men are taking paternity leave, but usually for a shorter time period.
I, myself worked less, and no overnights, while my kids were young. Eventually gradually increased back up to full time.
We should be very careful not to compare apples to oranges. One of the beauties of Emergency Medicine is the flexibility it offers, particularly to women.
I am all for income equality. Women make great doctors. The two items I don’t see addressed are days worked and patients seen. A lot of women want to work 3 days per week and have more family time.
All of the physicians included in the survey were “full-time.” Of course, full-time could be 40 hours/week or 80 hours/week. They did not seem to address that or any measure of productivity.
[…] Physician Compensation 2020: How Much Money Do U.S. Doctors Make Per Year? […]